Location: Home >> Detail
Pharm Front. 2019;1:e190003. https://doi.org/10.20900/pf20190003
 ,
Marilyn Casha 3,
Anton Grech 4,
Benjamin Micallef 2,
John Joseph Borg 2,
Anthony Serracino Inglott 1,2,
Godfrey LaFerla 3
,
Marilyn Casha 3,
Anton Grech 4,
Benjamin Micallef 2,
John Joseph Borg 2,
Anthony Serracino Inglott 1,2,
Godfrey LaFerla 3
1 Department of Pharmacy, Faculty of Medicine and Surgery, University of Malta, Msida, MSD 2080, Malta
2 Medicines Authority, Malta Life Sciences Park, San Ġwann, SĠN 3000, Malta
3 Department of Surgery, Faculty of Medicine and Surgery, University of Malta, Msida, MSD 2080, Malta
4 Department of Psychiatry, Faculty of Medicine and Surgery, University of Malta, Msida, MSD 2080, Malta
* Correspondence: Luana Mifsud Buhagiar, Tel.: +00356-79709140.
Background: Treatment guidelines in neuropathic pain list amitriptyline as a first-line option. Modest evidence on efficacy and safety concerns possibly shape the rationale behind dosing recommendations. An observational study was carried out to understand the usefulness of safety monitoring for this established medicine.
Methods: Twenty-six (26) subjects were categorized into 2 groups: 13 patients under pain management receiving 10 mg amitriptyline daily for less than 12 months, and 13 patients under psychiatric care receiving a daily dose of 25–75 mg for over 12 months. Dose-related reference ranges were calculated and blood levels were assessed for the case examples presented. Adverse events and ECGs were collated. QT intervals were corrected using Bazett’s and Fridericia’s formulae. Side-effect frequencies were evaluated both within the research groups, and in the broader perspective of spontaneous ADR reporting through EudraVigilance.
Results: The applicability of dose-related reference ranges, considering confounding factors such as drug interactions and metabolizer status, is discussed. Patients in both groups reported on average three side-effects, with drowsiness being reported more significantly in the 10 mg group and possibly attenuating with time; an observation not replicated for dry mouth. ADR reports with non-granulated information limit the usefulness of the data retrieved. Comparison of QT corrected with Bazett’s and Fridericia’s formulae suggests that Bazett’s may overestimate the number of patients on amitriptyline with QTc prolongation.
Conclusions: This research supports the adoption of evolving research observations to understand the implications of dosing recommendations and safety assessments in attempt of delivering individualized treatment with minimal risk.
ADR, adverse drug reaction; CHMP, Committee for Medicinal Products for Human Use; CMDh, Co-ordination group for mutual recognition and decentralised procedures—human; ECG, electrocardiogram; EV-DAS, EudraVigilance Data Analysis System; FDA, Food and Drug Administration; HIV, human immunodeficiency viruses; IASP, International Association for the Study of Pain; ICSR, Individual Case Study Report; SmPC, Summary of Product Characteristics; SNRI, serotonin and noradrenaline reuptake inhibitor; TCA, tricyclic antidepressant.
Neuropathic pain is “caused by a lesion or disease of the somatosensory system”, in contrast to the nociceptive origin of chronic pain arising from damage to non-neural tissue [1]. Population prevalence of pain with neuropathic properties is estimated to be around 7–10 percent [2], although indications point towards 20 percent of adults in Europe being potentially affected [3]. The origin of neuropathic pain is complex with known causes including diabetic neuropathy, postherpetic neuralgia, amputations, trauma, and HIV infection. Notwithstanding the diversity in aetiologies, neuropathic pain is considered as a distinct clinical entity.
Tricyclic antidepressants (TCAs), particularly tertiary amines like amitriptyline, are the most effectively studied antidepressants for the treatment of neuropathic pain. Pain relief is achievable at lower doses than those entailed in the treatment of depression, and is believed to be independent of the antidepressant effects of these drugs [4,5]. Multiple mechanisms are possibly involved, at central and peripheral locations, with amitriptyline modulating nociceptive and sensory processes at the receptor and ion channel level [6]. Postulations range from the effect on serotonin and noradrenaline along descending spinal pain pathways, to the influence of TCAs on histamine receptors, the modulation of sodium channels [7], and the differential regulation of opioid receptors [8].
Updated guidance from the Neuropathic Pain Special Interest Group of the International Association for the Study of Pain (IASP) recommends TCAs, serotonin and noradrenaline reuptake inhibitors (SNRIs), pregabalin, and gabapentin as first-line therapy. The systematic review and meta-analysis by Finnerup et al. [9] concluded that 16 out of the 18 placebo-controlled trials, evaluating amitriptyline in a daily dose of 25–150 mg, were positive. At the low doses prescribed for the control of pain, adverse effects, particularly sedation and dry mouth resulting from the anti-muscarinic activity of amitriptyline, were still reported [10].
Amitriptyline is readily absorbed in the gastro-intestinal tract, widely distributed throughout the body, metabolized in the liver and excreted in the urine. Systemic exposure is expected to be linear and predictable [11], albeit population pharmacokinetics and interpatient variability in the blood concentrations of amitriptyline and its metabolites may be influenced by the activity of cytochrome P450 subfamily enzymes, particularly CYP2C19 and CYP2D6, which are known to be subject to genetic polymorphism. The metabolic implications are further complicated by drug-drug-gene interactions occurring when another drug in the patient’s regimen affects the individual’s enzyme activity pertinent to amitriptyline, triggering potential predisposition to treatment failure or adverse events. Amitriptyline is the most anticholinergic antidepressant [12] and is associated with weight gain, sexual dysfunction, orthostatic hypotension and cardiotoxicity.
The long list of drugs that cause QT prolongation features amitriptyline which has been implicated with the specific form of ventricular tachycardia known as torsades de pointes [13]. Upward et al. [14] reported ECG changes which included shortened sinus cycle length with doses of 150–200 mg amitriptyline daily, together with an 8% and 10% prolongation of the PR interval and QRS duration, respectively. TCAs prolong the QTc predominantly by blocking the Na+ channel [15] with the effect being more pronounced by the inhibition of outward K+ channels [16]. Although ECG changes are most evident in over-dosage, it is suggested that tricyclic antidepressants may unmask subclinical dysfunctional sodium channels and trigger drug-induced sudden death in patients receiving chronic treatment [13].
Since heart rate has a biophysical effect on the QT interval, formulae, commonly Bazett’s square root formula or Fridericia’s cube root formula, may be used for QT correction. Bazett’s prevails as the most popular route for obtaining QTc, despite Fridericia’s correction possibly being more precise at the extremes of physiological heart rate [13], as may be the case in patients receiving TCA therapy [17,18]. A number of published studies evaluating QTc prolongation and amitriptyline use, either specify the use of Bazett’s formula in their methods, or lack details on which formula was used for QT interval correction [14,19–25]. Such array of data emerging in the literature and adverse events reported during the post-marketing period, as collated in the EU database of suspected adverse drug reactions (ADRs)—Eudravigiliance, serve to update the official sources of product information. The EU-CMDh (Co-ordination group for mutual recognition and decentralised procedures—human) published its scientific conclusions in 2015 [26] with amendments to be included in the relevant sections of the Summary of Product Characteristics (SmPC) involving a warning on “QT interval prolongation”, and “electrocardiogram QT prolonged” as a common adverse reaction. The US-FDA drug label for amitriptyline [27] also makes reference to cardiovascular adverse reactions and potential ECG changes.
The US-FDA label differs from the SmPC for amitriptyline in the EU particularly with respect to the indications, with the former solely listing “the relief of symptoms of depression”. Following a review completed by the EU-CHMP (Committee for Medicinal Products for Human Use) in 2017, the harmonised prescribing information for amitriptyline in the EU also includes “treatment of neuropathic pain in adults” as a therapeutic indication. The assessment report [28] concludes that the evidence for specific conditions cannot be considered sufficient but was not deemed to preclude a general indication in neuropathic pain. This was reflected in the SmPC whereby, for neuropathic pain, the posology presents as follows: Recommended doses are 25–75 mg daily in the evening. Doses above 100 mg should be used with caution. The initial dose should be 10–25 mg in the evening. Doses can be increased with 10–25 mg every 3–7 days as tolerated. The dose can be taken once daily, or be divided into two doses. A single dose above 75 mg is not recommended. The analgesic effect is normally seen after 2–4 weeks of dosing. There appears to be emphasis on a gradual increase in the dose of amitriptyline to the lowest effective dose, in attempt of enhancing tolerability and attenuating side-effect severity.
The 2017 CHMP assessment report [28] notes that twice daily dosing may be necessary for immediate release formulations, to limit sedation and ensure a 24-hour therapeutic coverage, possibly recognizing that the blood concentrations resulting from low-dose amitriptyline administered once daily potentially verge on sub-therapeutic. The latter may be particularly relevant for the 10 mg starting dose, which prescribers might feel most confident to adhere to over the proposed 2–4 weeks in which efficacy may be assessed, even though in the studies implicated to support the use of amitriptyline in the treatment of neuropathic pain, a 10 mg daily dose is somewhat unobserved [29–37]. This study aimed to investigate the safety rationale of using low-dose amitriptyline for neuropathic pain, through comparison with the reasonably higher doses administered in the management of depression. The implications of dose recommendations on blood levels and reported adverse events are discussed.
Outpatients of any gender, over 18 years of age, whose treatment plan includes the tricyclic antidepressant amitriptyline, were considered. The study population consisted of twenty-six (26) patients attending the psychiatric clinic or the pain clinic, suffering from depressive illness or neuropathic pain sufficiently severe to require therapy, with amitriptyline as monotherapy or as add-on, and follow up through the outpatients’ services of Mater Dei Hospital (MDH), Malta. Ethics approval for this study was granted by the University of Malta Research Ethics Committee in July 2017 (Ref. 23/2017). Written informed consent was obtained from all subjects before the study.
Subjects were categorized into two groups: thirteen (13) patients, being followed by a consultant psychiatrist, who had been receiving 25–75 mg amitriptyline daily for over 12 months; and thirteen (13) patients, being followed by a consultant anaesthetist, who had been receiving 10 mg amitriptyline daily for less than 12 months. Patients confirmed adherence to the prescribed dosing regimen upon questioning. Concomitant medications were noted, as applicable. Routine renal and liver function tests were performed throughout, whereas results of therapeutic drug monitoring and genotyping for CYP2D6 and CYP2C19 were made available as needed. Dose-related concentration (DRC) factors listed in the Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017 [38] were used to estimate the lower and upper limit of the expected dose-related concentration range, by multiplying DRC factors (low, −SD; high, +SD) by the daily dose.
The self-report Antidepressant Side Effect Checklist (ASEC), designed as part of the GENDEP project [39], which focuses on side-effects that have been previously associated with antidepressants, was utilized for compiling responses on adverse events [40]. Permission to use ASEC in this research was granted by The Royal College of Psychiatrists, London, UK. Patients were guided to score the 21 items indexed in ASEC, on a four-point scale (0 absent; 1 mild; 2 moderate; 3 severe), making note on whether the symptom was linked to amitriptyline. All patients underwent an electrocardiographic (ECG) examination, and each 12-lead ECG report was analyzed for heart rate, PR, QRSd, and QT corrected by the Bazett’s and Fridericia’s formulae.
In attempt of reviewing the safety outcomes from a pharmacovigilance perspective, all Individual Case Study Reports (ICSRs) for amitriptyline and “dry mouth” or “sedation” as Preferred Terms (PTs, distinct descriptors for symptom/sign), were extracted, on 6 March 2019, from the EU database on ADRs—EudraVigilance, using the EudraVigilance Data Analysis System (EV-DAS). Adverse drug reaction (ADR) data retrieved was rationalized to determine the number of reports for dry mouth and for sedation, according to the daily dose administered. Reports which did not specify the dosage of amitriptyline were excluded from the dataset.
Data analysis was conducted using Excel (Microsoft, WA) and SPSS Statistics 25 software (IBM Corporation, USA). Variables were reviewed using standard descriptive statistics and data distribution was evaluated for normality by the Shapiro-Wilk test. Pearson correlation test was used to explore relationship between continuous variables (e.g., heart rate and QTc). Fisher’s exact test was used when comparing categorical data (e.g., side-effect frequencies) in the two groups. The level of statistical significance was set at 0.05.
Twenty-six (26) patients, 5 males and 21 females, were categorized in two groups of 13 patients each, with comparable age (range: 24–79 years). Table 1 gives an overview of the cohort. The inclusion of patients receiving 10 mg amitriptyline daily facilitated comparison of a dose which is typically started with in pain management practice, as opposed to the higher doses prescribed in psychiatry, particularly with respect to safety implications. It is not intended to infer conclusions on the efficacy of amitriptyline doses for the diverse range of pain conditions, particularly in view that the pain scores reported by the 13 pain subjects (as an average intensity over the 4 weeks prior to assessment, scored on a scale from 0 to a maximum of 10) varied between 3 and 10 (median of 6) between subjects.
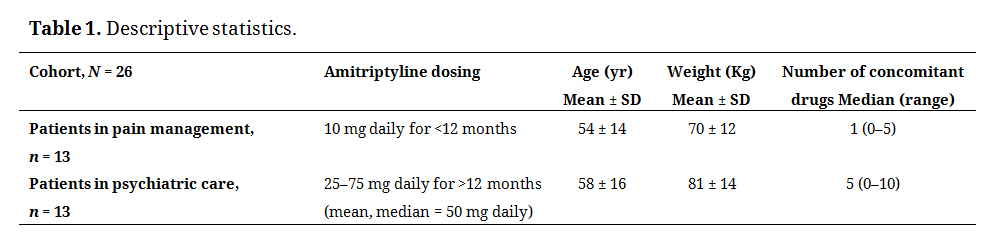 Table 1. Descriptive statistics.
Table 1. Descriptive statistics.
Published dose-related concentration (DRC) factors [38] were used to calculate the theoretically expected active moiety (amitriptyline + nortriptyline) concentration range for the relevant daily doses. The computed dose-related reference ranges and the therapeutic drug monitoring (TDM) concentrations observed in four of the subjects studied are reported in Table 2, as an example. Subjects 1–4 were identified on the basis of: (i) daily dose of 10 mg/25 mg/50 mg/75 mg; (ii) entire daily dose administered as one intake in the evening; (iii) steady-state achieved; (iv) blood withdrawn 12–15 hours after last dose for determination of concentrations in serum; (v) no significant hepatic or renal dysfunction; (vi) normal metabolizer phenotype determined from CYP2D6 and CYP2C19 genotyping. Normal metabolizer status for both the tested genes was reported for 14 patients (54%). The sample from 1 patient failed genetic testing and 11 patients (42%) had irregular metabolism reported for one or both genes. The case examples presented enable dose recommendations to be put into perspective with regards to the resulting blood levels in “normal” patients, without genetic polymorphisms or organ diseases impacting drug elimination. Other confounding variables, such as unreported non-adherence and drug interactions may still be present. Paroxetine was co-administered in 54% (7 out of 13) of the psychiatric patient population, whereas the 13 patients under pain management did not receive any concomitant CYP-inhibitors. This pharmacokinetic approach may be particularly relevant for amitriptyline in the management of neuropathic pain, since the lack of a widely accepted therapeutic reference range in the pain indication might render a pharmacodynamic approach less appropriate.
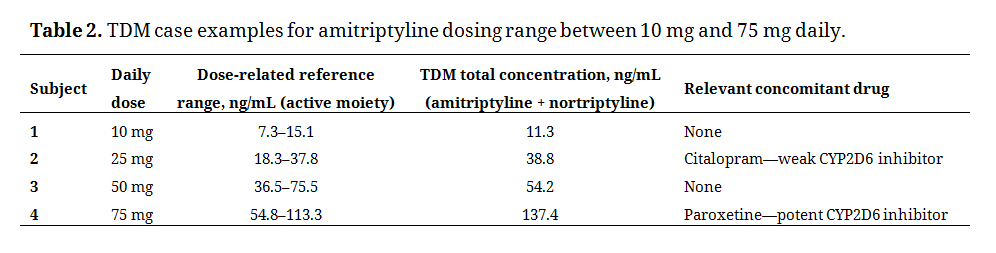 Table 2. TDM case examples for amitriptyline dosing range between 10 mg and 75 mg daily.
Table 2. TDM case examples for amitriptyline dosing range between 10 mg and 75 mg daily.
The ECG data was reviewed to identify potential: (1) PR interval prolongation, (2) widening of the QRS-complex, and (3) QT interval prolongation. In the assessment of the electrocardiographic reports, the PR interval was considered prolonged if >200 ms [41], the QRS-complex was considered widened if >120 ms [42], and the QTc interval was considered prolonged if >450 ms [43]. Figure 1(A) portrays QTc, as corrected by the Bazett’s formula (QTcB) and Fridericia’s formula (QTcF) for all patients, highlighting the differences between QTcB and QTcF as heart rate increases. Figure 1(B) depicts a significant correlation between the percentage difference QTcB–QTcF and heart rate (P < 0.01; Pearson correlation 1-tailed test). The data indicates that Bazett’s correction formula potentially underestimates QTc at heart rates below 60 bpm and overestimates QTc at elevated heart rates. Fridericia’s correction may be more appropriate in subjects with altered heart rates [43].
Considering QTcB, 6 subjects would be considered to have their QT prolonged (2 in the 10 mg group and 4 in the higher-dose group) while considering QTcF only one patient (in the higher-dose group) is considered to have QT prolongation. QRS-widening was observed in one (1) patient per group, while two (2) patients had prolonged PR (both patients from the 25–75 mg amitriptyline group). The PR interval was observed to be diminished with increasing heart rate, supporting a documented inverse relationship between the two [44,45].
Irrespective of the group—dose, duration of use, and indication—patients reported, on average, three (3) side-effects on ASEC which they associate to amitriptyline (median 3, range 0–8, in pain patients on 10 mg daily for less than 12 months; median 2, range 0–10, in psychiatry patients on 25–75 mg daily for over 12 months). Out of the 21 symptoms in ASEC, insomnia and decreased appetite (listed as uncommon and rare undesirable effects in the EU-SmPC, respectively) were the only two not reported by any of the subjects. The most reported side-effect overall was drowsiness (14 out of 26, 54%), with subsequent frequencies as follows: Drowsiness (54%) > Dry mouth (35%) > Blurred vision (19%) = Feeling like the room is spinning (19%) = Tremor (19%) > Constipation (15%) = Palpitations (15%) = Feeling light-headed on standing (15%) > Headache (12%) = Diarrhoea (12%) = Increased appetite (12%) = Problems with sexual function (12%) = Weight gain (12%) > Disorientation (8%) = Yawning (8%) > Nausea or vomiting (4%) = Problems with urination (4%) = Sweating (4%) = Increased body temperature (4%).
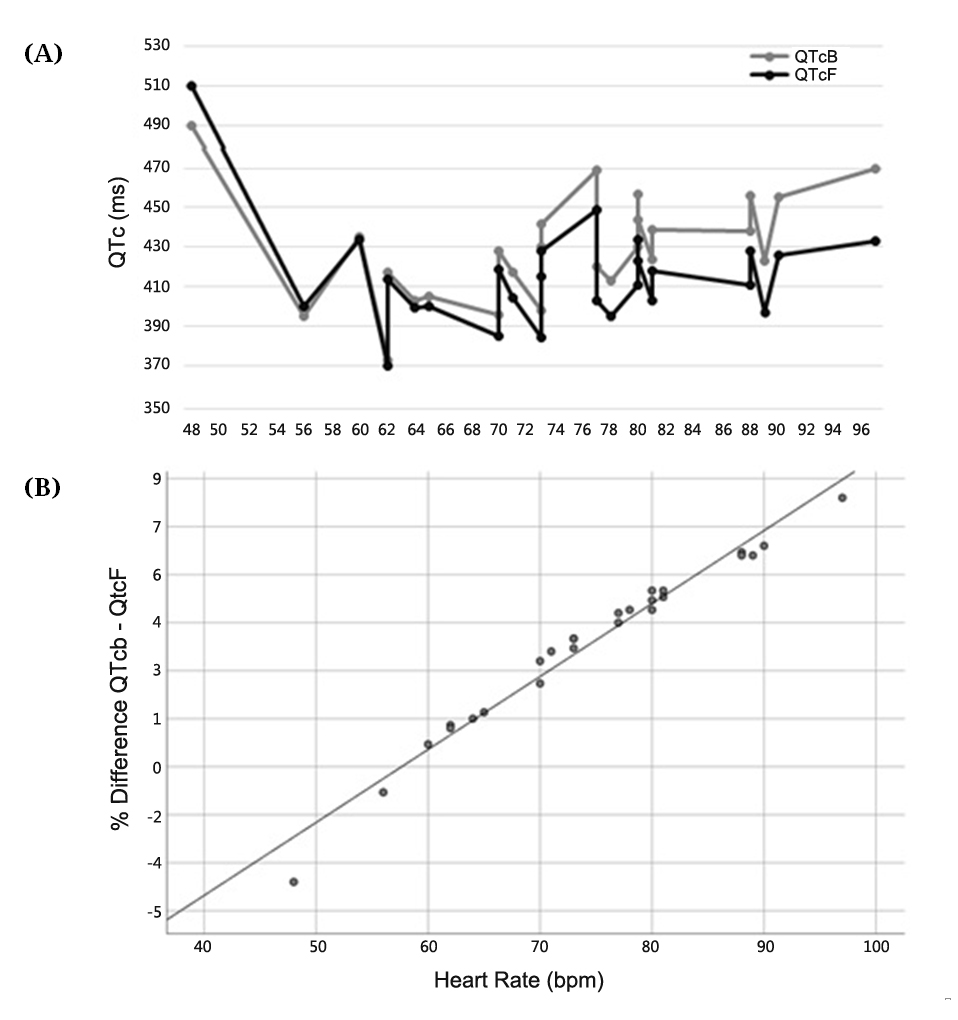 Figure 1. (A) QT corrected with Bazett’s formula (QTcB) and Fridericia’s formula (QTcF) for each patient vs. Heart Rate. (B) Percentage difference between QTcB and QTcF vs. Heart Rate.
Figure 1. (A) QT corrected with Bazett’s formula (QTcB) and Fridericia’s formula (QTcF) for each patient vs. Heart Rate. (B) Percentage difference between QTcB and QTcF vs. Heart Rate.
Drowsiness was reported more frequently in pain patients on 10 mg daily for less than 12 months (11 out of 13, 85%) compared to psychiatry patients on 25–75 mg daily for over 12 months (3 out of 13, 23%). Fisher’s exact test two-tailed P value of 0.0048 suggests that the latter observation is statistically significant. The frequency of drowsiness contrasts with dry mouth, which tended to be reported more by psychiatry patients receiving higher amitriptyline doses for a longer time-frame compared to pain patients on lower doses over a shorter course (6 out of 13, 46%; 3 out of 13, 23%; respectively). With respect to intensity, the highest reported score for dry mouth was 3 (severe), observed in 6 psychiatry patients and 1 pain patient, whereas for drowsiness the highest score reported was 2 (moderate), observed in 2 psychiatry patients and 9 pain patients.
Spontaneous Safety ReportsA total of 391 Individual Case Study Reports (ICSRs) were retrieved from EV-DAS; 310 ICSRs for amitriptyline and PT “dry mouth” and 81 ICSRs for amitriptyline and PT “sedation”. A total of 164 cases of dry month were reported in patients on a daily amitriptyline dose of 10 mg (54, 32.9%) or 25–75 mg (110, 67.1%). A total of 28 cases of sedation were reported in patients on a daily amitriptyline dose of 10 mg (4, 14.3%) or 25–75 mg (24, 85.7%). The outcomes, as summarized in Table 3, point towards higher reporting rates of both dry mouth and sedation for patients receiving 25–75 mg amitriptyline daily, as compared to a 10 mg daily dose. The patient population receiving 25–75 mg daily doses is possibly larger in size than that of patients prescribed 10 mg daily, which may in turn affect the estimates, just as could be the case for the numerous reports with unknown dose.
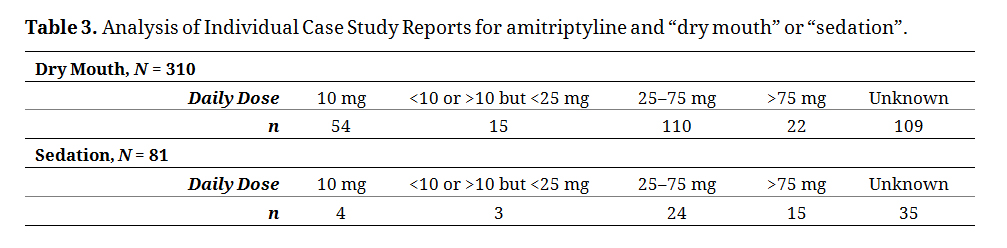 Table 3. Analysis of Individual Case Study Reports for amitriptyline and “dry mouth” or “sedation”.
Table 3. Analysis of Individual Case Study Reports for amitriptyline and “dry mouth” or “sedation”.
Attempts to establish a therapeutic window for amitriptyline analgesia endured as distant as decades ago [46]. A number of randomized controlled trials identify 75 mg per day as the average effective amitriptyline dose in the treatment of neuropathic pain [47], with blood levels of the active moiety close to 100 ng/mL [5]. As for safety, an upper concentration limit of 350 ng/mL has long been reported, below which a patient’s risk for serious undesirable complications is low [48]. Retrospectively, TCAs in dosages below 100 mg per day showed no increase in the risk of sudden cardiac death [49].
A 2015 Cochrane review [50] emphasized that good-quality evidence on the use of amitriptyline in neuropathic pain management is not clear and alluded to potential overestimation of efficacy. Looking into the studies considered by the research groups of both Moore [50] and Finnerup [9], amitriptyline is often initiated with a 12.5–25 mg dose, with subsequent increments. This might not be replicated in routine clinical practice whereby caregivers tend to continue prescribing amitriptyline at a daily maintenance dose as low as 5–10 mg per day, cognizant, or possibly over-cognizant, of the safety concerns [51]. Gradual dose titration is facilitated by the availability of scored dosage forms, and thus practical considerations with respect to the accessible strengths may not be a major concern. The recent review of IASP’s Neuropathic Pain Special Interest Group (NeuPSIG) on drug treatment for neuropathic pain underlines amitriptyline for first-line use and describes it as the most studied tricyclic antidepressant (TCA), in daily doses between 25 and 150 mg, with no evident dose-response effect. Multidimensional review of efficacy and adverse events is suggested in adopting a pragmatic approach whereby the TCA is initiated for 12 weeks, which is the ceiling duration studied in most trials, and thereafter withdrawn if there is no benefit. The recommendations are made in recognition that studies were marked by potential publication bias, large placebo effect and modest drug effects [52].
The CHMP 2017 assessment report [28] notes that slow titration of amitriptyline doses shall attenuate severity of sedation and dry mouth, among other side-effects, and increase tolerability. This may explain the rationale of recommending a markedly low starting dose. Our results indicate that sedation may indeed become less problematic in the long-term, even if there is dose escalation. In the case of dry mouth, however, it appears to persist over months of amitriptyline use and is perceived to interfere sufficiently in the patients’ quality of life to merit reporting. This questions the notion that anticholinergic adverse effects of amitriptyline generally abate with continued treatment, and favors the consideration that anticholinergic symptoms may fluctuate in their occurrence [53] or tolerance does not necessarily develop during long-term medication [54].
Does the lack of a recognized therapeutic range for amitriptyline in neuropathic pain warrant starting therapy with one-fifth of the initial dose recommended in depressed adults, to be on the safe side? Should this be the approach adopted, clinicians must be guided with respect to the necessary examinations and apt assessment measures, expected chronology, inter- and intra- patient confounding factors, and possibly also the reporting tools available to enable informed developments in safety appraisals. The supposition that clinical outcomes correlate better with blood levels than doses delineates the scope of therapeutic monitoring [55,56]. As illustrated by the case examples presented in this paper, dose-related reference ranges may be used, independently of a therapeutic reference range, to identify potential pharmacokinetic abnormalities which may impact on a patient’s systemic exposure to amitriptyline [38]. Blood levels outside the expected range may serve as an alert to actively look for disease-related changes, altered drug excretory functioning, and gene polymorphisms or drug-interactions that trigger ultra-rapid or poor metabolism, as may be the case with citalopram and paroxetine, at different levels [57]. Practical considerations, such as time, provider burden and pharmacoeconomics, although outside the scope of this text, may certainly influence the implementation prospects of the approach discussed whereby the cost of sampling, genotyping and monitoring blood levels approximated to around 170 Euro per patient. Irregular metabolism may not only influence the concentrations of amitriptyline and nortriptyline in blood, but also those of hydroxy metabolites that are potentially cardiotoxic [58] —an added concern which should further encourage ECG monitoring.
The International Conference on Harmonisation (ICH) Guideline E14 acknowledges the controversy over the most accurate QT correction available and recommends that corrections are performed using both the Bazett’s and Fridericia’s formulas, enabling detection of relevant effects on the QT/QTc interval [43]. The comparison of QT corrected with Bazett’s formula (QTcB) and Fridericia’s formula (QTcF) performed in this study supports research showing that the most widely adopted formula—Bazett’s—underestimates at heart rates below 60 bpm and overcorrects QTc values at elevated heart rates [15,59,60], which may be particularly relevant for amitriptyline cases whereby Bazett’s may overestimate the number of patients with QTc prolongation leading to the medication being potentially withheld as a safety measure [61].
The use of Fridericia’s formula is recommended, particularly at high heart rate, and investigating QTc changes from baseline should provide better individualized patient monitoring. Our subjects were assessed at one point in time and categorized as having prolonged QTc or otherwise. This cannot be extrapolated to determine whether amitriptyline causes QT prologation, which, although it represents a recent safety warning added to the SmPC, is somewhat also controversial. Investigating QTc prolonging effects of TCAs in a sub-group from the Rotterdam study, Noordam and colleagues [62], demonstrated statistically significant QTc prolongation with amitriptyline, using Bazett corrected QTc interval, which was lost upon adjusting for the increase in heart rate. The authors inferred that Fridericia’s formula might be preferred and suggested prospective revision to the warnings put forward by regulatory bodies in that TCAs might not indeed be associated with QTc prolongation. The 2018 review by Rochester et al. [18] included mixed studies conducted in neuropathic pain in which no significant impact on QTc was seen [21] or amitriptyline was reported to have significantly prolonged the QTc interval [22], although to a lesser extent than observed with doses used in depression. Caution is recommended in generalizing data, with practical distinction between studies on QT prolongation in overdose or toxicity, as opposed to standard clinical use. Our results substantiate that the method of QT correction may be critical in the interpretation of the data.
Gender, age and confounding medical conditions or medications are known to impact on QT prolongation [18]. It is important to note that systematic causality assessment was not performed in the present study, either for prolonged-QT, or any of the adverse reactions considered. Thus, pre-existing causality or coexistent disease/drug causality cannot be ruled out. Spontaneous reporting databases, which could represent a very useful resource for post-marketing safety assessment, may be limited by the poor data quality within the reports. While the undemanding disposition of the ADR reporting system may help mitigate the manifestation of under-reporting, follow-up of cases through contact between regulatory authorities and reporters, may lead to collation of more complete data with corresponding significance for developing further our understanding of safety implications.
Robust evidence, which typically emerges from randomized controlled trials, is deficient with respect to the use of amitriptyline in the treatment of neuropathic pain, particularly in patients who may present with complex histories, multiple comorbid disease states and co-medications [63]. Exclusion of such patients and merely focusing on “normal” subjects makes direct application of emerging evidence problematic. Clinical outcomes are determined by how amitriptyline is used in everyday practice. Inadequacies in dosing regimens, lengths of therapy, concordance, consistent monitoring, and quality ADR reporting may impact the real-world evaluation of the balance between therapeutic benefits and safety risks.
This work provides supportive evidence on how evolving research observations may be practically applied to better understand the implications of dosing recommendations and safety assessments, even for established drugs. Further work is necessitated in developing the themes elucidated by this work. Modern-day science, generating exploitable individualized data, may mitigate the hesitation associated with the trial-and-error prescribing of amitriptyline and drive informed clinical judgement, coupled with sensible follow-up, aimed at alleviating pain with minimal risk.
LMB, ASI and GL designed and implemented the study together with AG, MC, JJB and BM. The data was analyzed and the paper was written with input from all authors.
The authors declare no conflict of interest.
This research was funded by the ENDEAVOUR Scholarships Scheme, Malta.
The authors thank Robert Xuereb, Department of Cardiology, MDH; Chris Barbara, Carmel Sammut and Doris Grima, Department of Pathology, MDH; as well as Kristina Vella and Kersty Axisa for logistical support.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
Mifsud Buhagiar L, Casha M, Grech A, Micallef B, Borg JJ, Serracino Inglott A, LaFerla G. Safety implications of low-dose amitriptyline in neuropathic pain. Pharm Front. 2019;1:e190003. https://doi.org/10.20900/pf20190003

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




