Location: Home >> Detail
Adv Geriatr Med Res. 2019;1:e190006. https://doi.org/10.20900/agmr20190006

1 Department of Radiation Oncology, Rutgers Cancer Institute of New Jersey, New Brunswick, NJ 08903, USA
2 Framingham Heart Study, Boston University School of Medicine, Framingham, MA 01702, USA
3 Department of Biostatistics, Boston University School of Public Health, Boston, MA 02118, USA
4 Department of Neurology, Boston University School of Medicine, Boston, MA 02118, USA
5 Center for Neuroscience, Department of Neurology, University of California-Davis, Sacramento, CA 95817, USA
6 Department of Anatomy & Neurobiology, Boston University School of Medicine, Boston, MA 02118, USA
7 Department of Epidemiology, Boston University School of Public Health, Boston, MA 02118, USA
8 New England Geriatric Research Education and Clinical Center, VA Boston Healthcare System, Boston, MA 02130, USA
9 Division of Aging, Department of Medicine, Brigham and Women’s Hospital, Boston, MA 02120, USA
10 Division of Medical Oncology, Dana Farber Cancer Institute, Harvard Medical School, Boston, MA 02215, USA
* Correspondence: Jane A. Driver, Tel: +1-617-525-7946; Fax: +1-617-525-7739.
Background: Previous studies have demonstrated a strong inverse association between cancer and risk of Alzheimer’s disease (AD). This study aimed to further investigate this association by examining measures of cognitive performance and neuroimaging.
Methods: Neuropsychological (NP) test batteries consisting of quantitative measures of memory and executive function and volumetric brain magnetic resonance imaging (MRI) scans measuring brain and white-matter hyperintensity volumes were administered to 2043 dementia-free participants (54% women) in the Framingham Heart Study (FHS) Offspring cohort from 1999 to 2005. History of cancer was assessed at examination visits and through hospital records. Linear regression was used to examine the association between cancer history and NP/MRI variables.
Results: There were 252 and 1791 participants with and without a previous history of cancer, respectively. Cancer survivors had an average time between diagnosis and NP/MRI exam of 9.8 years. History of any invasive cancer was associated with better executive function (Beta = 0.16, p = 0.04) but not memory function. Non-invasive cancer was not associated with any change in cognitive performance. Patients with prostate cancer had larger frontal brain volumes (Beta = 4.13, p = 0.03). Cancer history was not associated with any other MRI measure.
Conclusions: We did not find any strong evidence linking cancer to cognitive or neuroimaging biomarkers that would explain a lower risk of subsequent AD, although a previous FHS study demonstrated a strong inverse association between cancer and risk of AD. Future work should examine the association between cancer and other biomarkers of AD as well as more sensitive metrics of AD-related brain aging markers.
A large body of evidence suggests an unusual relationship between cancer and neurodegenerative disorders [1,2]. Recent epidemiologic studies have found that a history of cancer is associated with a 35%–60% reduced risk of Alzheimer’s disease (AD), and similarly, AD is associated with a 12%–71% reduced risk of overall cancer [3–8]. These findings are not entirely due to survival bias, as they are seen both in survivors and non-survivors, and the inverse association is seen both before and after diagnosis of either disease [5]. Several meta-analyses have confirmed the association [9,10]. In contrast to its relationship with AD, cancer is not associated with a lower risk of vascular-type dementia, and in fact has been positively associated with the development of cerebrovascular disease [3,8]. Such an inverse association is biologically plausible, as AD and cancer share a number of genes and pathways that are expressed in opposite directions [11].
While these findings are intriguing, epidemiologic studies of the association between two severe age-related diseases are innately complex [12], and it is difficult to adequately account for bias and confounding [13]. That a history of cancer might protect against AD also seems counterintuitive because cancer treatments, and cancer itself, have been associated with cognitive impairment [14–16]. Furthermore, there is substantial positive overlap between the two conditions, including dysregulation of energy metabolism, inappropriate entry into cell cycle, inflammation and oxidative stress.
What is needed to take this investigation further are studies that determine whether markers of AD or cancer provide substantive evidence of this inverse comorbidity at a structural and functional level. A number of studies have shown that magnetic resonance imaging (MRI) markers of structural brain aging and performance on neuropsychological tests correlate with the later development of clinically-apparent dementia [17–20]. However, studies looking at how these markers relate to cancer incidence have reported disparate findings. While some have found that faster cognitive decline is associated with decreased risk of cancer mortality, others have shown long-term cancer survivors to have increased cognitive dysfunction [21,22]. A study in the Alzheimer’s disease Neuroimaging Initiative (ADNI) confirmed the inverse association between cancer and AD but did not see any MRI findings to suggest that cancer survivors have any evidence of neuroprotection [23].
Prior work from the Framingham Heart Study (FHS) found a strong bi-directional inverse relationship between cancer and AD [8]. If cancer is somehow “neuroprotective” for those who survive it, then it might be reflected in known AD endophenotypes. Specifically, we hypothesized that cancer survivors might have fewer deficits on cognitive tests that are associated with AD as well as increased brain volumes. We therefore investigated the association between a history of cancer and neuropsychological (NP) measures of cognitive performance and quantitative MRI markers of brain aging in the community-based Framingham Offspring cohort.
The study included participants from the FHS Offspring cohort [24], consisting of 5124 persons who have been examined approximately every four years since 1971. Participants were eligible for inclusion if they had at least one parent in the original FHS cohort or were the spouse of a biological Offspring participant. Participants who attended the seventh Offspring clinic examination (n = 4379) were invited to take a NP test battery and undergo volumetric brain MRI from 1999 to 2005. A total of 2223 participants completed NP testing and underwent MRI in the time period of one year before and five years after the seventh Offspring clinic examination. We excluded participants with prevalent dementia, stroke, or other neurological conditions at the time of testing (n = 83), missing education (n = 2), and a diagnosis of cancer within 5 years prior to NP/MRI testing (n = 95). Thus the final sample for the current analysis consisted of 2043 participants. This study was approved by the FHS Research Committee (ID# 2014.2022; September 29, 2014) and all participants provided signed consent at the time of health and NP examinations.
Cancer AssessmentHistory of cancer was assessed at each examination. If participants missed an examination, updates on health history were obtained through postal surveys and telephone interviews. Local hospital admission records and death records were also monitored for ascertainment of cancer cases. Once a case was identified, two independent people reviewed the patient’s medical record to confirm the diagnosis. Fewer than 3.4% of diagnoses were based solely on death certificates or clinical assessment, as pathology and operative reports were used to confirm the majority of cases [25]. We examined the presence of any cancer, as well as the following cancer subtypes: basal/squamous skin cancer, any cancer excluding basal/squamous skin cancer, prostate cancer, and breast cancer. If a participant had a diagnosis of more than one type of cancer, they could appear in multiple cancer subgroups. Multiple occurrences of the same cancer subtype were counted as a single occurrence of cancer.
Outcome Assessment Cognitive functionParticipants were administered a NP test battery as a quantitative measure of cognitive performance. The battery included the delayed recall components of the Logical Memory (LM-D), Visual Reproduction (VR-D), and Verbal Paired Associates (VPA-D) subtests of the Wechsler Memory Scale. Also included were the Halstead-Reitan Trailmaking Test B (Trails B), the Hooper Visual Organization Test (HVOT), and the Similarities subtest of the Wechsler Adult Intelligence Scale (Similarities). Standard test administration and scoring procedures, as described in previous FHS publications, were used [26].
Structural brain agingBrain MRI techniques used in the FHS have been described previously [27]. Briefly, a 1 or 1.5-T Seimens Magnetom scanner was used to acquire three-dimensional T1 and double echo proton density and T2 coronal images in 4-mm contiguous slices. Centralized reading of all images was performed (QUANTA 6.2, Sun Microsystems Ultra 5 Workstation). Total cerebral brain volume (TCBV), frontal brain volume (FBV), temporal brain volume (TBV), and temporal horn volume (THV) were calculated. All measures are expressed as a percentage of total cranial volume to adjust for head size. Also computed was white matter hyperintensity volume (WMHV). To identify white matter hyperintensities, the first and second echo images from T2 sequences were summed and a segmentation threshold was determined as 3.5 standard deviations in pixel intensity greater than the mean of the fitted distribution of brain parenchyma [28]. This technique has been previously validated [29].
Covariate MeasurementThe following variables were assessed at the seventh Offspring clinic examination: diabetes, hypertension, history of cardiovascular disease (CVD), current cigarette smoking, and APOE4 carrier status.
Statistical AnalysesDescriptive statistics (mean, median, frequency) were calculated for all outcome variables. HVOT, Trails B, THV, and WMHV were natural log (ln) transformed to improve normality. Linear regression models were constructed to examine the association between cancer history (any cancer, basal/squamous skin cancer, any cancer excluding basal/squamous skin cancer, prostate cancer, and breast cancer) and each of the NP and MRI outcomes. All cancer groups were compared to a common referent group of participants with no history of cancer. For all regression models, ln Trails B was re-signed so that higher scores indicate better performance, to be consistent with the directionality of the other NP tests. Model 1 adjusted for age, sex, education (no high school degree, high school degree, college degree, greater than college degree), and time interval between cancer exposure and NP/MRI exam. Model 2 was further adjusted for cardiovascular risk factors (hypertension, diabetes, history of cardiovascular disease, smoking), and ApoE4 carrier status (presence of ≥1 ApoE4 alleles). All models for the MRI outcomes were additionally adjusted for age-squared due to the non-linear association between age and brain volume measures [27]. A p-value of <0.05 was considered statistically significant. All statistical analyses were performed using SAS version 9.4 (Cary, NC, USA).
Table 1 presents the baseline characteristics of the 2043 participants included in the analysis. There were 252 and 1791 participants with and without a previous history of cancer, with a mean age of 67.4 years (SD = 8.0 years) and 60.8 years (SD = 9.2 years) at time of NP/MRI exam, respectively. Cancer survivors had an average time between their first diagnosis of cancer and NP/MRI exam of 9.8 years (SD = 7.5 years). The range of years over which the cancer diagnoses were made was 1958–2003, with the median year of diagnosis being 1992. Sex distribution, prevalence of diabetes, and ApoE4 carrier status were similar between both groups, while those with a history of cancer were less likely to hold a college degree (34.5% vs. 40.1%), had a lower prevalence of smoking at time of assessment (7.1% vs. 13.1%), and had a higher prevalence of hypertension (49.2% vs. 40.0%) and history of CVD (15.5% vs. 9.1%). Cancer survivors also had higher non-corrected WMHV.
 Table 1. Study sample characteristics (N = 2043).
Table 1. Study sample characteristics (N = 2043).
Table 2 presents the distribution of cancer types. The largest sub-group of cancers was basal and squamous skin cancers (60.5%), followed by prostate cancer (9.1%) and breast cancer (8.3%).
 Table 2. Distribution of cancer types.
Table 2. Distribution of cancer types.
Table 3 presents the association of cancer history with NP measures. None of the cancer types showed a statistically significant association with either LM-D or VR-D, measures of verbal and visual memory, respectively. However, history of any cancer excluding basal/squamous skin cancer was associated with lower scores for VPA-D (Beta = −0.67, p-value = 0.02), a test of verbal learning and memory.
Tests of executive functioning showed a positive response. Similarities, which tests abstract verbal reasoning among other cognitive abilities, showed a positive association—those with a history of prostate cancer had significantly higher scores than those without any cancer (Beta = 4.64, p-value = 0.04). History of any cancer showed a statistically significant positive association with Trails B, a widely-used test of overall executive function (Beta = 0.11, p-value = 0.01). History of any cancer excluding basal/squamous skin cancer and history of breast cancer were also associated with better Trails B scores (Beta = 0.16, p-value = 0.04 and Beta = 0.54, p-value = 0.004, respectively). Additionally, none of the cancer types were associated with HVOT, a measure of visuoperceptual abilities.
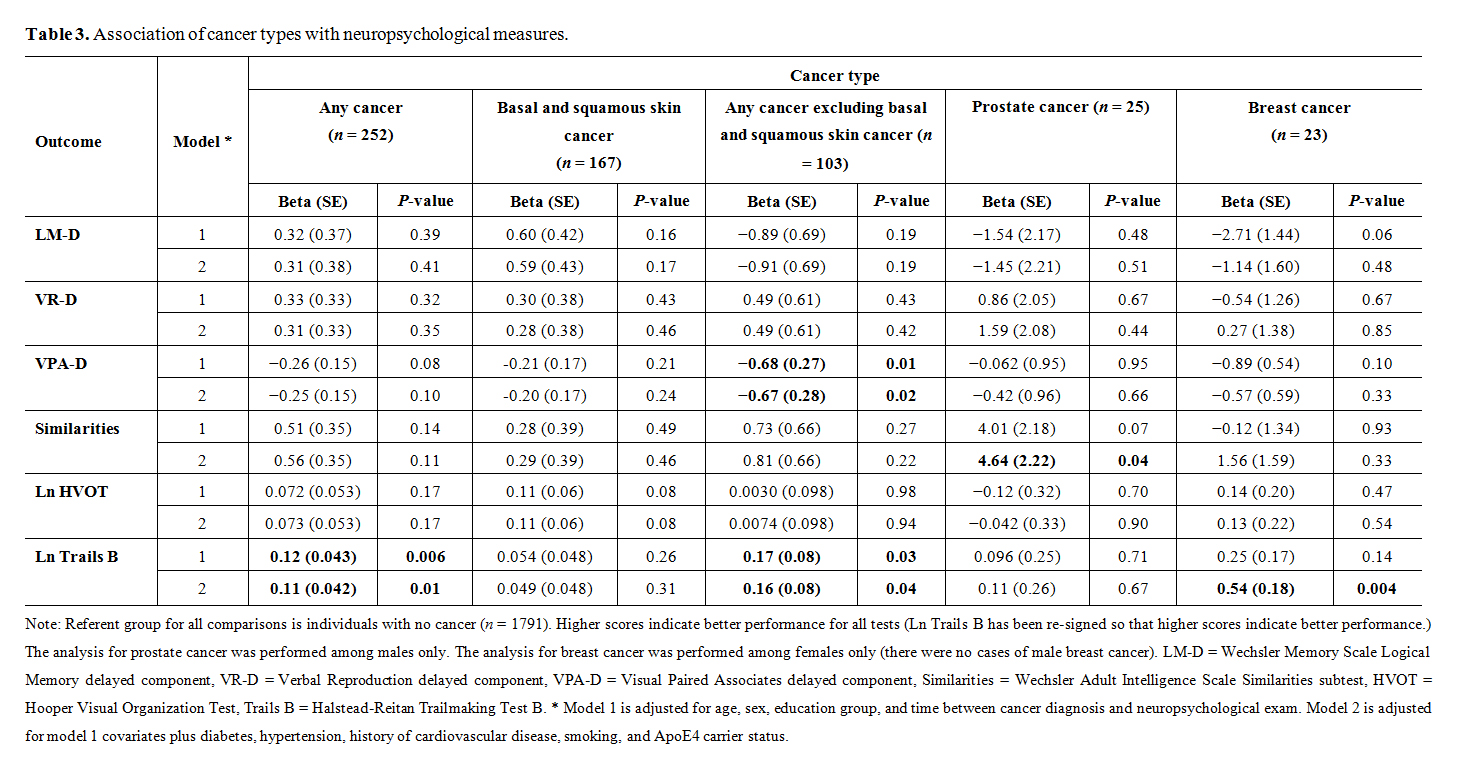 Table 3. Association of cancer types with neuropsychological measures.
Table 3. Association of cancer types with neuropsychological measures.
 Table 4. Association of cancer types with MRI measures.
Table 4. Association of cancer types with MRI measures.
Table 4 presents the association between cancer and MRI markers. There were no associations found between any of the cancer types and total cerebral brain volume, temporal brain volume, temporal horn volume, or white matter hyperintensity volume. Those with a history of prostate cancer were found to have significantly larger frontal brain volumes than those without any history of cancer (Beta = 4.13, p-value = 0.03).
In this analysis of the FHS Offspring cohort, we did not find any strong evidence linking a history of cancer to neuropsychological or MRI measures that have been associated with increased AD risk. Survivors of invasive cancer types, including the largest cancer sub-types of prostate and breast cancer, had statistically significant better performance in various measures of executive function. This association was not evident in those with a history of non-invasive cancer types (basal/squamous skin cancer) as expected. There was also an isolated finding of those with any invasive cancer having a memory decrement on one of three memory tests. Among the MRI variables that were tested, survivors of prostate cancer were also found to have larger frontal brain volumes.
Overall these results are intriguing in that they show cancer survivors to have modestly better executive function, rather than memory, compared to their non-cancer peers. This is particularly interesting as prior work showed a strong inverse relationship between cancer and AD/dementia within the FHS population. In a prospective analysis including 1274 members of the original FHS cohort, cancer survivors were found to have a 33% decreased risk of developing probable AD [8]. Likewise, in a case-control analysis including 1,198 members of both the original and offspring FHS cohorts, patients with probable AD and any type of dementia had a 61% and 56% decreased risk of developing cancer, respectively [8]. Given that these results have been replicated in other large epidemiological studies [3–7], the notion is that there are structural and functional substrate level changes that underlie or explain these observed protective effects. That we found better preclinical executive function may illustrate the heterogeneity of AD and would align with a potential vascular etiology consistent with Zlokovic’s two-hit vascular hypothesis and the increasing evidence of a preclinical vascular pathway to AD [30].
Further, the inverse epidemiological association between some cancers and AD has led to an examination of the genetic and biologic links between the two conditions [31]. A common theory posits that neurodegeneration and cancer lie at opposite ends of the same spectrum, with cell senescence and apoptosis dominating at one extreme and cellular over-proliferation and tumorigenesis at the other. Pin1, Wnt, and the ubiquitin proteasome system are examples of proteins and pathways that are differentially up-regulated in one disease and down-regulated in the other [11,32–35]. Further, bioenergetic models have proposed that fundamental differences in the energy metabolism of cycling cells and neurons may promote one condition while protecting from the development of the other [36].
Nudelman et al., in the ADNI cohort, found that cancer survivors had a measurable delay in AD onset independent of APOE status; the magnitude of the delay increased with the number of prior cancers in a “dose-response” pattern [23]. However, cancer survivors did not have any regions of increased cortical gray matter density (GMD) on MRI to suggest the possibility that their neurons were more likely to survive. In fact, cancer survivors had lower GMD in the right superior frontal gyrus compared to non-cancer survivors. This area is not usually affected early in AD, but has been associated with a history of cancer and cancer treatment. These effects were only seen in participants with a history of invasive cancer, and not in basal and squamous skin cancer.
Adding to the unknown biological connection is evidence that cancer can cause cognitive dysfunction, which suggests that separate mechanisms may be in play for indirect, beneficial effects secondary to cancer’s protection from neurodegeneration versus direct, adverse cognitive effects from cancer itself. Cancer has been associated with global decreased white matter volume prior to the initiation of any treatment, correlating with neuropsychological studies that show an association with increased processing deficits [37]; however, other studies have not shown any structural differences at baseline [38]. Additional studies have found that patients with cancer have increased pre-treatment frontoparietal activation compared to healthy controls [15,39], especially in prefrontal regions, suggesting a subtle working memory impairment and recruitment of additional brain areas for compensation. Our finding of a decrement in the verbal learning task in the absence of other memory test differences may reflect this working memory impairment. Cancer treatments, such as chemotherapy and hormonal therapy, have also been extensively studied for their impact on brain structure and function. Multiple studies have shown receipt of chemotherapy to be related to diffuse decrease in gray and white matter volume, generally persisting long-term after treatment is completed [16,38]. Functional MRI studies related to working and verbal memory tasks have found regions of hypoactivation, especially in the prefrontal cortex, inferior frontal cortex, medial temporal lobe, and posterior parietal cortex, at up to more than 10 year post-treatment [40,41], although one study found a return to pre-treatment baseline at one year [15]. Similarly, receipt of hormonal therapy has been found to be associated with worse performance on tests involving learning, memory, executive function, and processing speed [42], with deficits lasting over the long-term, but formal tests involving MRI imaging remain to be pursued.
Strengths of our study include its measurement of cancer, cognition, and structural brain imaging in a well-defined cohort with long-term follow-up. Our lack of information on cancer treatment is a major limitation, as we are not able to look specifically at those who received chemotherapy or hormonal therapy. Another limitation is the small sample sizes for individual cancer types, limiting any conclusions that can be drawn for these groups. It should be emphasized that our study focuses on the results of cognitive population screening, and we excluded those diagnosed with clinical dementia and other neurologic disorders, leaving a study sample that was biased toward little to no cognitive impairment. Further, the study sample is highly educated and predominantly white, limiting the generalizability of these results to other ethnic or racial groups.
What we can conclude is that in this cohort of healthy middle-aged adults, there is insufficient evidence to relate history of invasive cancer with better indices of cognitive or neuroimaging markers. This is particularly interesting when considered alongside studies that show protective benefits of cancer on AD and dementia. Future work should examine the association between cancer and other biomarkers of AD including β-amyloid, tau, and markers of inflammation and neuronal metabolism, as well as more sensitive metrics to changes in cognition and neuroimaging, particularly related to white matter integrity.
The dataset of the study is available from the authors upon reasonable request.
AG, study contribution and design, interpretation of data, drafting and revision of manuscript for intellectual content. SRP, study design, acquisition of data, analysis and interpretation of data. AB, analysis and interpretation of data. GLS, acquisition of data, revision of manuscript for intellectual content. CD, interpretation of data, revision of manuscript for intellectual content. RA, study contribution and design, interpretation of data, revision of manuscript for intellectual content, study supervision. JAD, study contribution and design, interpretation of data, drafting and revision of manuscript for intellectual content, study supervision.
The authors declare that there is no conflict of interest.
This work was supported by the Framingham Heart Study’s National Heart, Lung, and Blood Institute contract (N01-HC-25195) and by grants from the National Institute of Neurological Disorders and Stroke (R01 NS17950) and from the National Institute on Aging (R01 AG16495; AG08122). Dr. Driver is funded by VA Merit Review Award I01CX000934-01A1. The funding sources were not involved in study design, data collection and interpretation, manuscript preparation, or the decision to submit the work for publication.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
Gupta A, Preis SR, Beiser AS, Splansky GL, DeCarli CS, Au R, et al. Relationship of Cancer to Brain Aging Markers of Alzheimer’s Disease: The Framingham Heart Study. Adv Geriatr Med Res. 2019;1:e190006. https://doi.org/10.20900/agmr20190006

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




