Location:Home >> Detail
J Psychiatry Brain Sci. 2016; 1(5): 2; https://doi.org/10.20900/jpbs.20160020

1 The Mental Health Center and the Psychiatric Laboratory, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, China
2 Department of Biology Products, American Informatics Consultant LLC, Rockville, MD, 20852, USA
3 Spark Energy LLC, Houston, TX 77253, USA
First Author: Qing Gao, The Mental Health Center and the Psychiatric Laboratory, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, China.
Joint First Author: Zhe Li, The Mental Health Center and the Psychiatric Laboratory, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, China.
*Corresponding Author: Guyu Zhang, Spark Energy LLC, Houston, TX, 77253, USA; Tel:225-304-1636.
Background: Recently, several studies reported possible association between gene FKBP5 and schizophrenia (SCZ). Their results suggested that FKBP5 may link to stress and cognition in case of SCZ, which warranted further study in the field.
Method: In this study, we performed a systematical literature review, focusing on FKBP5--brain region association studies and brain region--SCZ relations, with the purpose of identifying potential FKBP5 → brain → SCZ pathogenic pathways.
Results: We identified over 1,500 references supporting the relation of four common brain regions that related to both FKBP5 and SCZ. These brain regions include hypothalamus, hippocampus, prefrontal cortex, amygdaloid. Analysis showed that FKBP5 affects the structure and function of these four brain regions with different mechanisms, which may in turn influence the pathogenesis of SCZ.
Conclusion: Our results support the hypothesis that FKBP5 present linkage to the development of SCZ, which help to gain better understanding of the underlying FKBP5 → SCZ association mechanism.
Schizophrenia (SCZ) is one of the most chronically disabling psychiatric illnesses with a global median lifetime morbid risk of 7.2/1000 persons[1]. Early manifestations of the illness often appear in mid to late adolescence, with clinical onset typically following 2-5 years later. In clinical settings the disorder is identified through the presence of impairments across several clusters of symptoms, namely positive, negative, and cognitive symptoms, disorganization, altered mood and motor symptoms. Although etiology of SCZ remains unclear, recent neuroimaging studies provide compelling evidence of abnormalities of cerebral structure and function in patients with SCZ[2-4]. For instance, reductions in the volume of the hippocampus and the amygdala are consistent findings in imaging studies of SCZ[5], while enlarged hypothalamic volumes in SCZ have also been identified[6]. Moreover, SCZ patients tend to present functional dysconnectivity within/between several brain regions, including prefrontal cortex, hypothalamus, hippocampus, and amygdaloid[6-10]. These studies suggest that the genes linked to functional or structural changes of these SCZ-related brain regions are worthy of further study.
The protein encoded by gene FKBP5 is a member of the immunophilin protein family, playing roles in immunoregulation and basic cellular processes involving protein folding and trafficking. This gene is a key molecule in the stress response and the pathophysiology of psychiatric symptoms. Studies showed that FKBP5 plays a role as a glucocorticoid receptor (GR) regulator, influencing the GR binding and translocation by binding and initiating intracellular feedback on the GR system[11]. FKBP5 inhibits the function of GRs, which regulate adrenocortical secretion of glucocorticoids during stress-induced Hypothalamic pituitary adrenal (HPA) axis activity. The activation of the HPA axis is controlled through a negative feedback mechanism -- by the activation of GRs at different levels of FKBP5[12,13]. Under the pathological conditions, the function of the HPA axis is disrupted, and this may eventually lead to structural and functional changes in brain regions[14,15].
The HPA-axis-regulation function of FKBP5 has been confirmed later by other studies, which were observed within many brain regions[12]. It has been demonstrated that HPA axis is directly involved in inducing mood behavior after chronic social defeat stress[16]. These findings explain the results from some other genetic studies that linked FKBP5 with posttraumatic stress disorder, depression and anxiety[17-19]. For instance, Yehuda et al. found that the single nucleotide polymorphisms (SNPs) in FKBP5 interacts with childhood trauma and could be used to predict severity of adult posttraumatic stress disorder (PTSD)[18].
On the other hand, HPA axis dysregulation is suggested as one of the possible mechanisms related to the vulnerability-stress model of SCZ[20], posing a functional linkage between FKBP5 and SCZ. As a matter of fact, several recently studies reported possible association between the genetic changes of FKBP5 with the stress and cognition in case of SCZ[20-22]. However, further studies are need on exploring the functional mechanisms of FKBP5 that affect the pathogenic development of SCZ.
In this study, we conducted a systematically review on the association between FKBP5 and the brain regions, abnormalities of which are related to SCZ. Our study identified four potential FKBP5 → brain regions → SCZ pathogenic pathways through which FKBP5 influence the symptoms and development of SCZ.
The literature reference selection criteria is described as follows. We searched the whole PubMed abstracts and approximately 4M+ Elsevier full journal papers, looking for two groups of papers: first, papers describing relationships between FKBP5 and its related brain regions; second, papers reporting SCZ related brain regions. There are 20 brain regions demonstrated functionally relation with FKBP5, and 134 brain regions related to schizophrenia. Then, we further selected the ones from these references that contain brain regions associated with both FKBP5 and SCZ. We identified four brain regions that demonstrate upstream regulations with FKBP5 (FKBP5 →Brain Regions), meanwhile downstream regulation with SCZ (Brain Region → SCZ). After manually inspection, we finally picked up 1,561 references and present them in Supplementary Data, including the titles and related sentences where these FKBP5-gene or SCZ-gene were identified. These references include 129 papers reporting relationships between FKBP5 and 4 brain regions (i.g., hypothalamus, Hippocampus, prefrontal cortex, amygdaloid). Also included are three references claim direct linkage between SCZ and FKBP5. The rest 1,428 references are these supported relationships between SCZ and the four brain regions mentioned above. Our study identified four gene → brain → disease pathogenic pathways, as shown in Fig 1 The detailed description of the construction of these pathways are presented in the following sections.
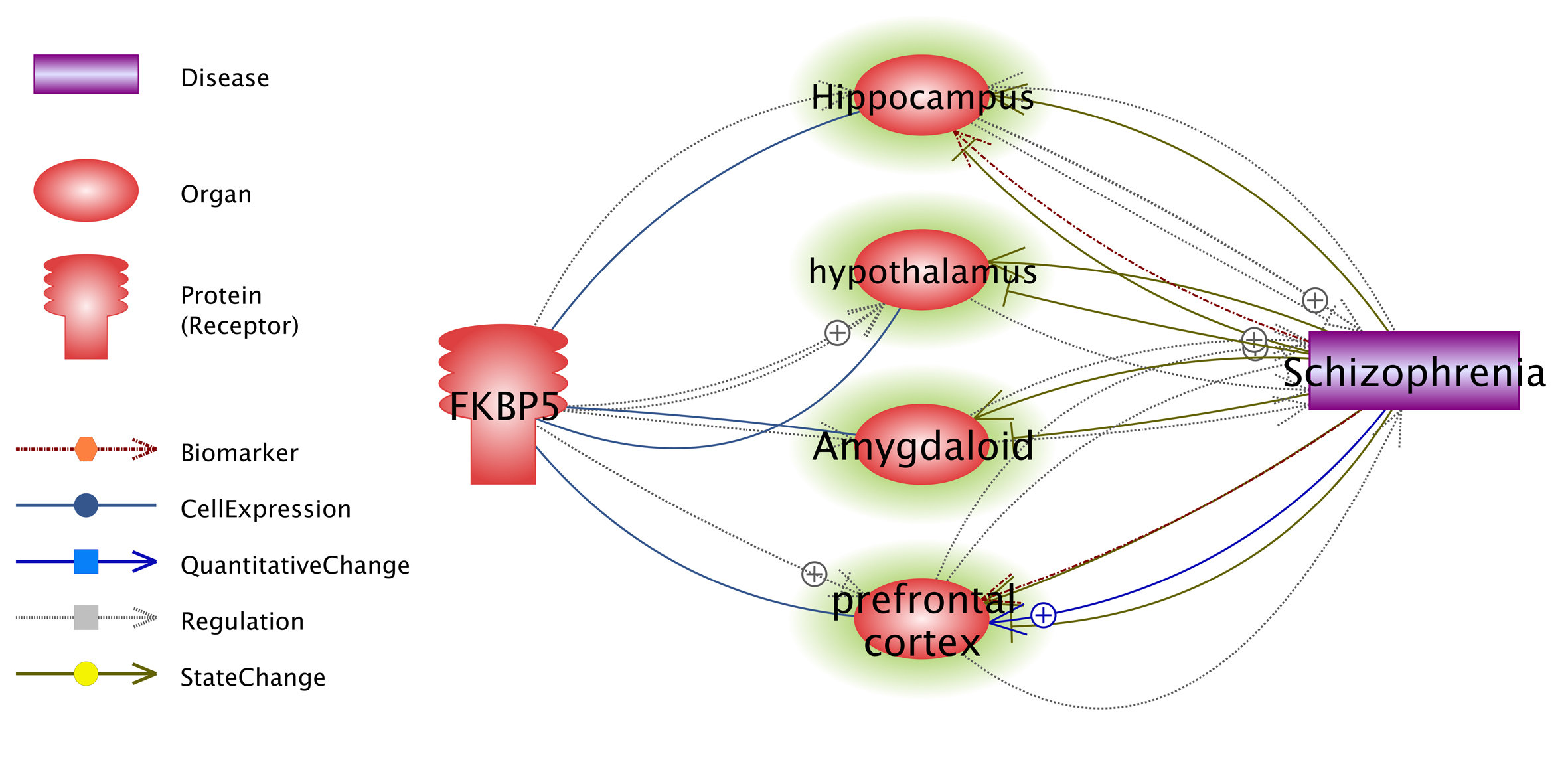
Fig. 1 Possible FKBP5 → brain → SCZ pathogenic pathways identified through systematic literature review. The four brain regions were highlighted in green.
In this section, we present the detailed discussion on four potential FKBP5 → brain → SCZ pathogenic pathways. These pathways may contribute to a better understanding of the mechanisms of how FKBP5 could play roles in the pathogenic development of SCZ. The four brain regions involved in the discussion are hypothalamus, hippocampus, prefrontal cortex, amygdaloid. All these brain regions demonstrated strong association with SCZ, both functionally and structurally.
2.2 FKBP5- Hippocampus-SCZHippocampus is a major component of the brains regions of humans and other vertebrates, which is densely populated with glucocorticoid receptors (GRs)[23]. Studies showed that persistent dysregulation of GR subcellular distribution is predicted to damage the hippocampal formation[24]. Highly expressed in the hippocampus, FKBP5 has been shown to regulate the steroid receptor function, including progesterone, androgen, and GRs[11]. By altering GR sensitivities, FKBP5 influences the function and morphology of hippocampal[25]. It has been identified that FKBP5 expression in hippocampus is also linked to reduced short term memory[26], altered cortisol negative feedback[27] and chronic mild stress (CMS)[28].
On the other hand, studies indicated that functional abnormalities in the hippocampus, as well as hippocampal volume reductions may be a vulnerability marker for SCZ [10, 29-32]. Therefore, structural deficits or dysfunction in the hippocampus resulted from the alteration of FKBP5 expression and GRs could build up a possible FKBP5 → Hippocampus → SCZ pathway linking FKBP5 to SCZ.
2.3 FKBP5-hypothalamus-SCZ pathwayHypothalamus is a portion of the brain that contains a number of small nuclei with a variety of functions. One of the most important functions is to link the nervous system to the endocrine system via the pituitary gland (hypophysis). FKBP5 has been suggested as one of the key modulators of hypothalamic pituitary adrenal axis (HPA axis)[33-35], which controls reactions to stress and regulates many body processes, including digestion, the immune system, mood, emotions, sexuality, energy storage and expenditure. The activation of the HPA axis is controlled through a negative feedback mechanism, by the activation of GRs at different levels of FKBP5[12,13]. For example, Albu et al. found that FKBP5 plays an important regulatory role in the HPA axis necessary for stress adaptation and recovery[33]. Fujii et al. also suggested that FKBP5 variant (rs1360780) regulates HPA axis reactivity and expression levels of GR[34], which regulate adrenocortical secretion of glucocorticoids during stress-induced HPA axis activity. Other studies shown that chronic treatment with corticosterone mediates behavioral changes caused by stress possible through increasing FKBP5 mRNA expression[36] and altering FKBP5 methylation in the hypothalamus [37]. Animal models of stress also highlighted a role for FKBP5 in mediating coping behaviors to stress and in the mediation of stress effects[38-40].
Both functional and structural changes of hypothalamic have been linked to SCZ. For example, abnormalities in HPA axis has been found to play a role in the clinical manifestation of SCZ[41]. Enlarged hypothalamic volumes in schizophrenia were found SCZ patients compared to controls[6]. These findings suggest a HPA axis regulation based FKBP5 → hypothalamic → SCZ pathogenic pathway.
2.4 FKBP5- prefrontal cortex-SCZPrefrontal cortex covers the front part of the frontal lobe. This brain region has been implicated in planning complex cognitive behavior, personality expression, decision making, and moderating social behavior[42]. Both functional and/or structural abnormality of prefrontal cortex could lead to SCZ like performance in neural networks, and may account for pathological working memory in the disorder. The aberrant changes within prefrontal cortex linked to SCZ include: alterations in information processing in prefrontal cortex[43], a reduction of prefrontal cortical hubs[44], abnormal dopamine release within the brain region[45,46], the neural circuitry abnormality[47], and reduced dendritic volume of prefrontal cortical neurons[5]. Moreover, many studies noted that connectivity of the prefrontal cortex is reduced in schizophrenia, particularly for intra-prefrontal cortex connectivity [8,9].
Meanwhile, studies showed that FKBP5 is associated with both functional changes and physical alterations of prefrontal cortex. For example, decreased FKBP5 expression[48] and disrupted GR-mediated signaling pathway along with HPA axis hyperactivity resulted in neuronal atrophy in the dorsolateral (dl) - and dorsomedial (dm) - prefrontal cortex and subsequent mood-related behavior alterations[49]. Wei et al. found that exposure to chronic mild stress led to a markedly upregulated FKBP5 protein expression in the prefrontal cortex[50]. Further, deletion of FKBP51 has been suggested to play a role in preventing stress-induced prefrontal cortical synapsin loss[21]. All these studies provided evidence for the functional and structural regulation relationship between FKBP5 and prefrontal cortex, supporting a potential FKBP5 → prefrontal cortex → SCZ pathogenic pathway. As a matter of fact, Basta-Kaim et al. confirmed that decreased activity of FKBP5 in the frontal cortex result in the HPA axis hyperactivity via altering GR function in SCZ[51].
2.5 FKBP5- Amygdala-SCZThe amygdala are two almond-shaped groups of nuclei located deep and medially within the temporal lobes of the brain, the primary role of which is in the processing of memory, decision-making, and emotional reactions. Functional and structural abnormalities of amygdala have been linked to SCZ emotion related symptoms. Some studies concluded that reduced amygdala activation[52] or implicate aberrant amygdala activity[53,54] may underlie deficits in emotion recognition in schizophrenia, which support the involvement of amygdala activation in the positive symptoms of schizophrenia. In addition, patients suffering from SCZ present reduced volumes of the amygdala, which is partially caused by the decreases in the number of synapses[55].
FKBP5 has been linked to emotional, memorial and learning behaviors via regulation within amygdala. For example, Attwood et al observed that overexpressed FKBP5 in the amygdala has a direct anxiogenic effects[56]. Hadamitzky et al. showed in an animal model that, increased neuronal activities as well as overexpression of FKBP51 in the amygdala seem to trigger anxiety-like behavior in naive rats[57]. Moreover, in a drug treatment study, Sawamura et al. reported that dexamethasone treatment was associated with reduced FKBP5 mRNA expression in the amygdala after extinction learning and retention[58]. Considering the pivotal role of the amygdala in mood regulation, associative learning, and modulation of cognitive functions, alteration of FKBP5 gene expression in the amygdala may contribute differentially to these abnormalities. Integrating these discussions, a FKBP5 → Amygdala → SCZ pathogenic pathway seems reasonable.
SCZ is a complex mental health disorder, whose pathophysiology is linked to structural abnormalities and functional deficits of many brain regions. Results from this systematic review showed that, FKBP5, a protein of the immunophilin family, plays roles within multiple brain regions that are linked to SCZ. Dysfunction of FKBP5 could lead to functional and/ or structural changes of these brain regions, namely hypothalamus, Hippocampus, prefrontal cortex, Amygdaloid. The variance of these brain regions in turn will influence SCZ relation brain functions, including GR-responsive pathways and HPA axis activities, mood, emotion, memory and learning related behavioral alterations. Our study built up multiple potential FKBP5 → brain → SZC pathways as possible causal regulating tunnels, through which FKBP5 influence the pathogenesis of SCZ. Results from this study help to understand the mechanisms underlying FKBP5 → SCZ association.
TThis study is partly supported by Science and Technology Department of Sichuan Province (2017SZ0049 , Zhe Li), and Health and Family Planning Commission of Sichuan Province (17PJ080, Zhe Li).
We would like to thank all authors for their contribution to the study.
The authors claims no conflict of interests.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
Gao Q, Li Z, Jones P, Zhang G. A Possible Role of the FKBP5 Gene in Schizophrenia. J Psychiatry Brain Sci. 2016; 1(5): 2; https://doi.org/10.20900/jpbs.20160020

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




